Using a peptide for belly fat isn't some fringe biohacking trend anymore. It's a clinically studied approach that's gaining serious traction among physicians and patients frustrated by midsection weight that won't budge, no matter how many crunches or calorie cuts they try.
Visceral fat, the deep abdominal fat packed around organs, is notoriously resistant to standard diet and exercise. It's also the most metabolically dangerous type of fat, linked to increased risk of heart disease, type 2 diabetes, and fatty liver disease. Traditional weight loss strategies often reduce subcutaneous fat (the pinchable kind) while leaving visceral stores largely intact.
That's where peptide therapy enters the picture. Specific peptides, from FDA-approved options like tesamorelin to GLP-1 receptor agonists like semaglutide and tirzepatide, work through distinct biological mechanisms to target stored belly fat. Some stimulate growth hormone release. Others suppress appetite at the brain level. A few do both.
This guide breaks down which peptides actually work for belly fat, what the clinical data says, realistic timelines for results, and what to know about side effects before starting treatment. It's part of the broader conversation about peptides for weight loss and how targeted options compare to general approaches.
What Are Peptides and Why Do They Target Belly Fat?
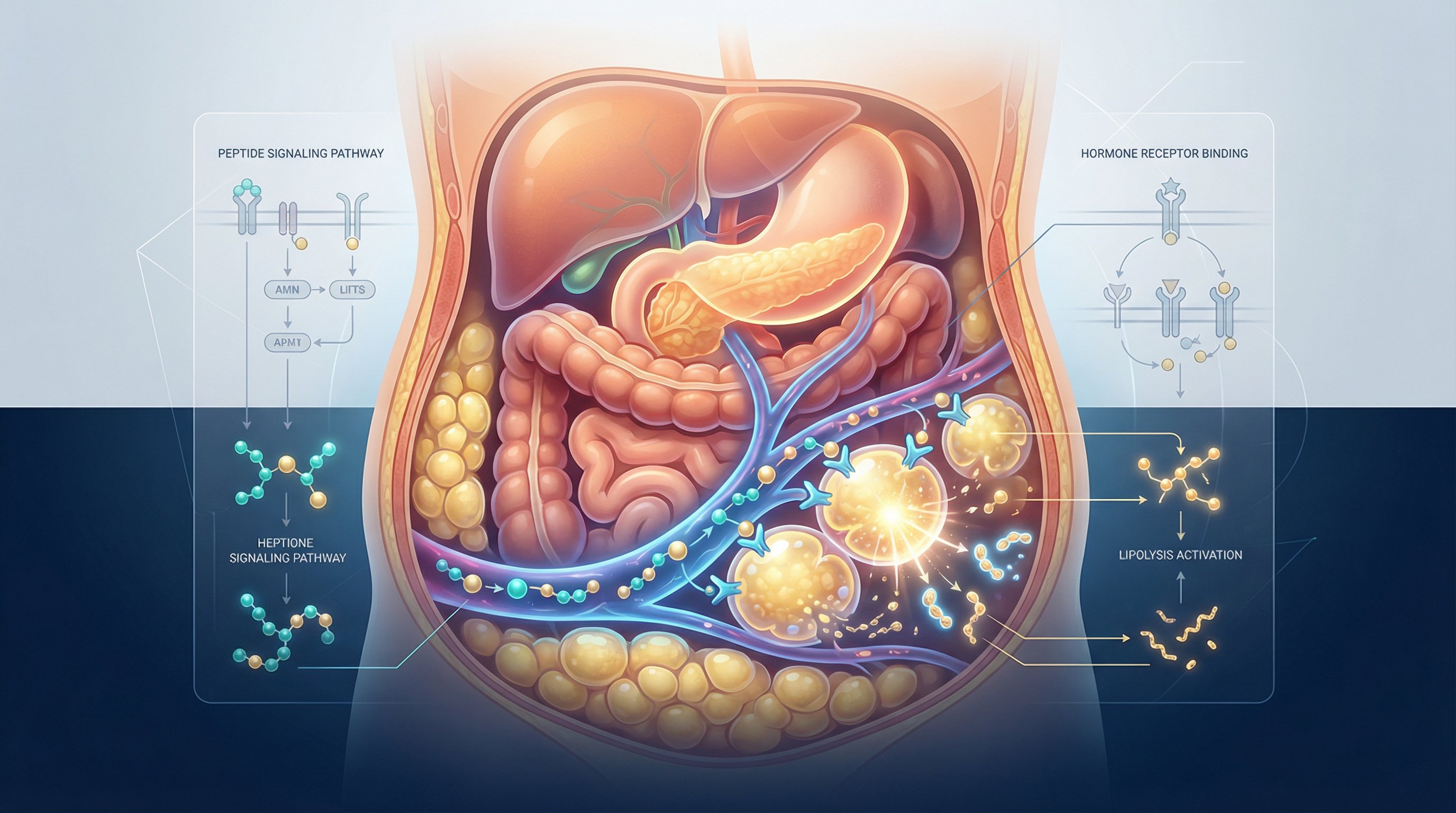
Peptides are short chains of amino acids, typically between 2 and 50, that act as signaling molecules in the body. They function similarly to hormones, binding to specific receptors to trigger biological responses. Unlike synthetic drugs designed from scratch, many therapeutic peptides mimic molecules the body already produces.
So why belly fat specifically?
Visceral adipose tissue (VAT), the fat surrounding organs in the abdominal cavity, has a uniquely high density of hormone receptors. This makes it more responsive to hormonal signaling than subcutaneous fat in areas like the thighs or arms. Peptides exploit this receptor density.
Here's how different peptide classes target belly fat:
- Growth hormone-releasing peptides (like tesamorelin and CJC-1295/ipamorelin) stimulate pituitary GH secretion, which activates lipase enzymes that break down stored triglycerides in visceral fat cells
- GLP-1 receptor agonists (like semaglutide and tirzepatide) act on brain receptors to reduce appetite while improving insulin sensitivity, which shifts the body away from fat storage
- Fat-fragment peptides (like AOD-9604) target fat metabolism pathways directly, though with considerably less clinical evidence
The key distinction is that visceral fat is metabolically active tissue. It responds to hormonal signals faster than other fat depots. A 2019 study published in The Journal of Clinical Endocrinology & Metabolism confirmed that growth hormone-releasing peptides preferentially reduce visceral fat while preserving lean muscle mass, a result standard calorie restriction rarely achieves.
This receptor-driven targeting is what separates peptide therapy for belly fat from generic weight loss approaches. Patients exploring semaglutide specifically may also want to understand compounded semaglutide options, which offer the same active ingredient at lower cost. Patients aren't just losing weight. They're losing it from the place that matters most for metabolic health.
Top Peptides Used to Reduce Belly Fat

Not all peptides work the same way, and not all have equal evidence behind them. Here's a breakdown of the most commonly used peptides for belly fat reduction, ranked by clinical support.
FDA-approved options with strong evidence:
- Tesamorelin – The only FDA-approved peptide specifically for visceral fat reduction (approved for HIV-associated lipodystrophy). Reduces VAT by approximately 11% versus placebo in clinical trials.
- Semaglutide (Wegovy/Ozempic) – GLP-1 agonist with 14.9% mean weight loss in the STEP 1 trial (1,961 patients, 68 weeks). Also demonstrated a 20% reduction in major cardiac events in the SELECT trial.
- Tirzepatide (Zepbound/Mounjaro) – Dual GIP/GLP-1 agonist achieving up to 22.5% weight loss in the SURMOUNT-1 trial. Currently the most effective approved single-agent therapy.
- Liraglutide (Saxenda) – First-generation daily GLP-1 agonist. Around 8% weight loss. Now available as a generic, making it the most affordable option in this class.
Investigational or off-label options:
- CJC-1295/Ipamorelin – Growth hormone secretagogue stack popular in anti-aging clinics. Boosts GH for fat metabolism and muscle preservation. Not FDA-approved for weight loss.
- Retatrutide – Triple receptor agonist (GIP/GLP-1/Glucagon) showing 28.7% weight loss in Phase 3 trials. Not yet commercially available: earliest approval estimated mid-2027.
- AOD-9604 – A fragment of human growth hormone. Some off-label use for fat reduction, but limited published clinical data.
Tesamorelin: The Leading Peptide for Visceral Fat
Tesamorelin deserves special attention because it's the only peptide with FDA approval specifically targeting visceral abdominal fat.
It works by binding to growth hormone-releasing hormone (GHRH) receptors in the pituitary gland. This triggers pulsatile GH release, mimicking the body's natural rhythm rather than flooding the system with constant GH levels. The released growth hormone then activates hormone-sensitive lipase, an enzyme that breaks down stored triglycerides in visceral fat cells.
The clinical results are specific and well-documented:
- ~11% reduction in visceral adipose tissue versus placebo in controlled trials
- Measurable waist circumference reduction within 12–26 weeks
- Preservation of lean muscle mass during fat loss
- Improvements in triglyceride levels and insulin sensitivity markers
What makes tesamorelin particularly interesting for belly fat is its selectivity. Unlike general weight loss interventions, tesamorelin doesn't significantly reduce subcutaneous fat. It preferentially targets the visceral depot, the metabolically dangerous fat that standard dieting often misses.
The standard protocol involves a daily subcutaneous injection of 2 mg. Most clinical trials ran 26 to 52 weeks. One important caveat: tesamorelin is currently FDA-approved only for HIV-related visceral adiposity. Off-label prescribing for general visceral fat reduction is growing but requires a knowledgeable provider.
For patients exploring peptide therapy options, platforms like Peptide Injections can match individuals with board-certified physicians who specialize in these protocols, often in under two minutes.
How Peptide Therapy for Belly Fat Actually Works
Understanding the mechanism matters. It helps set realistic expectations and explains why peptide therapy for belly fat often succeeds where diet alone fails.
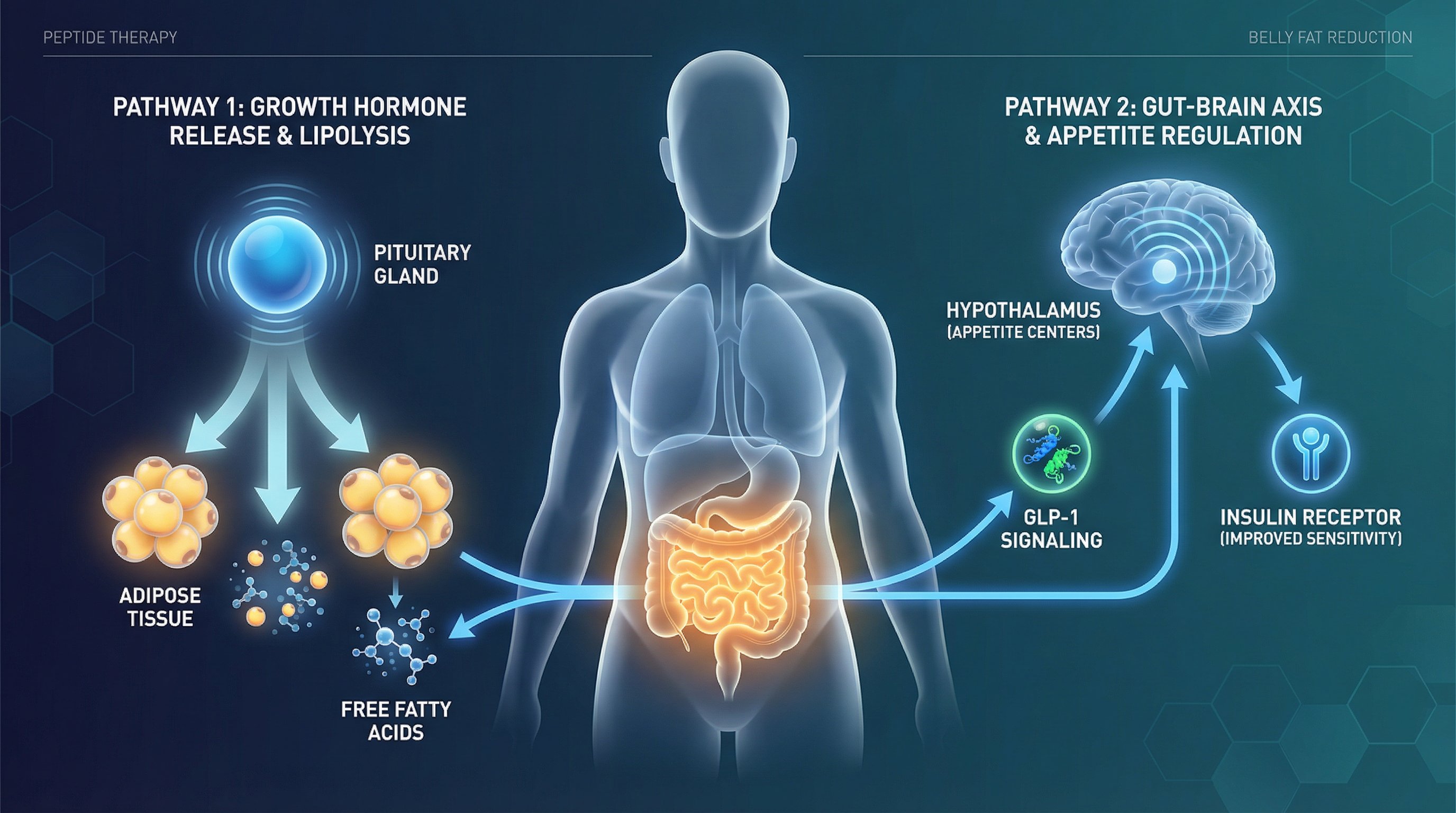
Growth hormone pathway (tesamorelin, CJC-1295/ipamorelin):
These peptides stimulate the pituitary gland to release growth hormone in natural pulses. GH then travels to adipose tissue, where it activates hormone-sensitive lipase. This enzyme breaks stored triglycerides into free fatty acids and glycerol, which the body can then burn for energy.
Visceral fat cells have more GH receptors per cell than subcutaneous fat cells. That's why GH-releasing peptides disproportionately affect belly fat. The process also boosts IGF-1 (insulin-like growth factor 1), which supports muscle protein synthesis, helping patients lose fat without losing muscle.
GLP-1 pathway (semaglutide, tirzepatide, liraglutide):
GLP-1 receptor agonists work differently. They mimic a gut hormone called glucagon-like peptide-1, which:
- Slows gastric emptying, so patients feel full longer after meals
- Acts on hypothalamic appetite centers, reducing hunger signals at the brain level
- Improves insulin sensitivity, shifting metabolic balance away from fat storage and toward fat oxidation
Tirzepatide adds a second mechanism by also activating GIP (glucose-dependent insulinotropic polypeptide) receptors, which partly explains its superior weight loss results compared to pure GLP-1 drugs.
The dual approach many clinicians prefer:
Some providers combine a GH-releasing peptide with a GLP-1 agonist. The logic is straightforward: one pathway directly breaks down visceral fat while the other reduces caloric intake and improves metabolic efficiency. This isn't standard protocol everywhere, and patients should only pursue combination therapy under direct physician supervision.
The biological reality is that belly fat didn't accumulate overnight and won't disappear overnight. But peptide therapy provides specific hormonal levers that diet and exercise alone can't pull. The body's own machinery does the work, peptides just provide the signal.
What Results to Expect and How Long They Take
Patients considering a peptide for belly fat naturally want to know: how much fat will I lose, and how fast?
The honest answer depends on which peptide, the starting point, and lifestyle factors. But clinical data gives us concrete benchmarks.
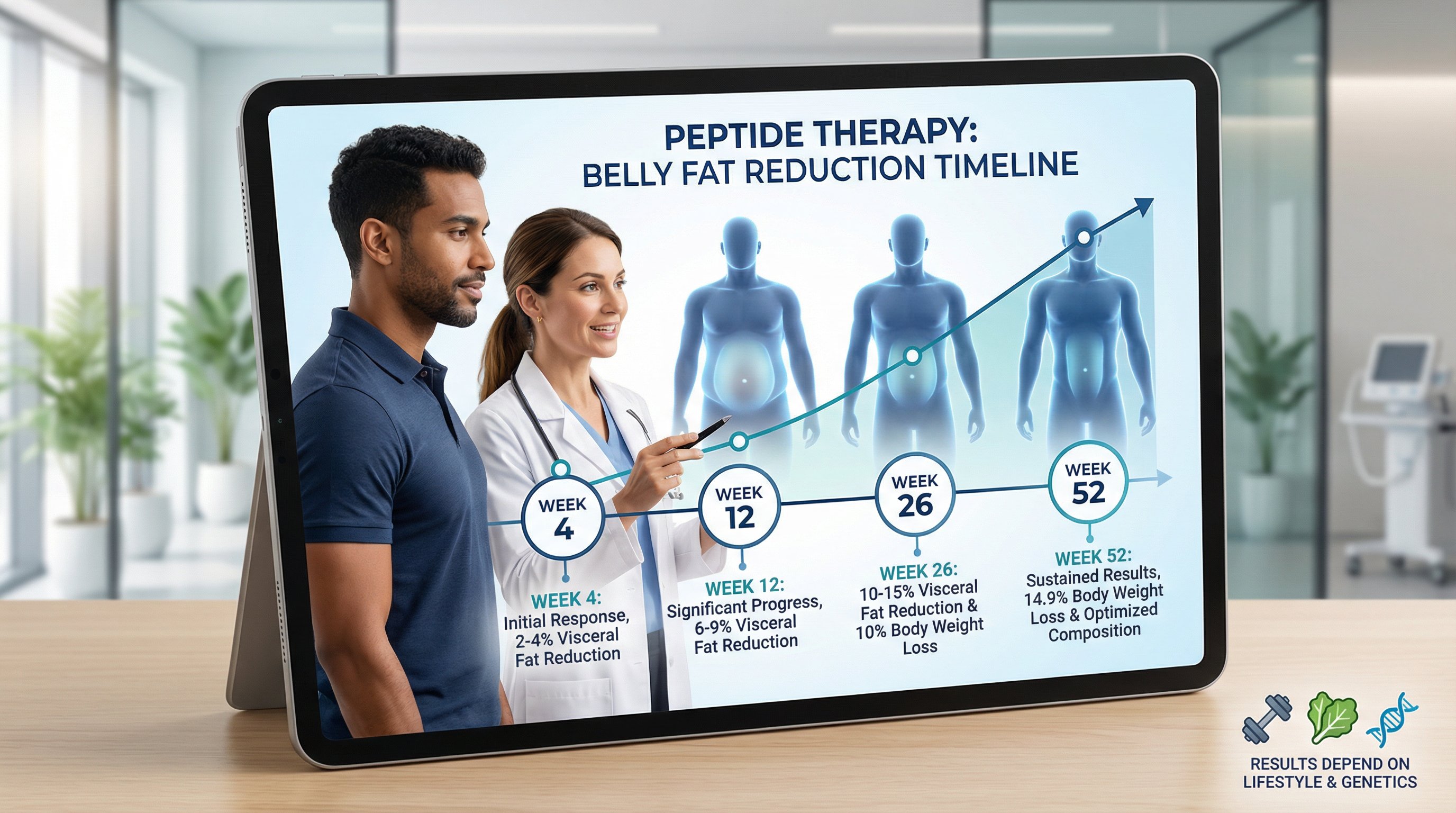
Tesamorelin timeline:
- Weeks 4–8: Subtle changes. Patients may notice improved energy and sleep quality before visible fat loss.
- Weeks 12–16: Measurable reduction in waist circumference typically becomes apparent. CT scans in trials showed significant VAT reduction by this point.
- Weeks 26–52: Full effect. Approximately 10–15% reduction in visceral fat with daily 2 mg injections.
GLP-1 agonist timeline:
- Semaglutide: 14.9% mean body weight loss at 68 weeks (STEP 1 trial). Most patients see 5% loss by weeks 12–16, with continued loss through month 12–15.
- Tirzepatide: Up to 22.5% body weight loss at 72 weeks (SURMOUNT-1). Faster early response than semaglutide in head-to-head comparisons.
- Liraglutide: More modest at ~8% body weight loss. Daily dosing. Results plateau around 6 months for most patients.
Important context on these numbers:
Clinical trial participants also followed structured diet and exercise programs. Peptide therapy alone, without lifestyle changes, produces significantly reduced results. Most physicians consider peptides an accelerator, not a replacement for healthy habits.
Weight regain is also a documented concern. The STEP 1 extension data showed that patients who discontinued semaglutide regained approximately two-thirds of lost weight within one year. This suggests peptide therapy for belly fat is often a long-term commitment rather than a short course.
Genetics matter too. Research shows that variants in genes like GLP1R, MC4R, and FTO influence how strongly patients respond. GLP1R A/A carriers may lose 3–5% more body weight on semaglutide, while MC4R risk carriers tend to plateau earlier. Platforms like Peptide Injections connect patients with providers who can evaluate these factors and recommend the right protocol from the start.
Safety, Side Effects, and Who Should Consider Peptide Therapy

Any honest discussion about peptide therapy for belly fat needs to address safety head-on. These are pharmaceutical compounds, not supplements.
Common side effects by peptide class:
GLP-1 agonists (semaglutide, tirzepatide, liraglutide):
- Nausea (up to 44% with semaglutide)
- Diarrhea (approximately 30%)
- Vomiting (24%)
- Constipation (24%)
- Decreased appetite (expected, but can become excessive)
Most GI side effects improve after the first 4–8 weeks and can be minimized with slow dose titration. Escalating too quickly is the most common cause of intolerable nausea.
GH-releasing peptides (tesamorelin, CJC-1295/ipamorelin):
- Injection site reactions (redness, swelling)
- Joint pain or fluid retention
- Mild tingling or numbness
- Elevated IGF-1 levels (requires monitoring)
Serious risks to know about:
- Pancreatitis – Rare but documented with GLP-1 agonists. Baseline amylase and lipase testing is standard before starting.
- Gallbladder events – Rapid weight loss from any cause increases gallstone risk. GLP-1 therapy is no exception.
- Medullary thyroid carcinoma (MTC) – GLP-1 drugs carry an FDA box warning based on rodent studies. Patients with personal or family history of MTC or MEN2 syndrome should not use these medications.
- Cancer risk with GH peptides – Theoretical concern that elevated IGF-1 could promote tumor growth. No causal link established in human studies, but patients with active malignancies should avoid GH-releasing peptides.
Who is a good candidate for peptide therapy?
- BMI ≥30 (or ≥27 with metabolic comorbidities like insulin resistance or elevated triglycerides)
- Significant visceral fat confirmed by waist circumference >40 inches (men) or >35 inches (women)
- Patients who've plateaued with diet and exercise alone
- Those with metabolic syndrome markers who need accelerated fat reduction for health reasons
Who should avoid it:
- Pregnant or breastfeeding individuals
- Patients with active cancer or history of MTC/MEN2
- Those with severe gastroparesis or history of pancreatitis
- Anyone with a diagnosed eating disorder
The single most important safety step is working with a qualified physician who understands peptide protocols, monitors bloodwork, and adjusts dosing based on individual response. This isn't something to self-prescribe from an overseas pharmacy.
Finding the right provider can be the hardest part. Peptide Injections was built to solve that problem, matching patients with board-certified physicians who specialize in peptide therapy, with personalized protocol recommendations based on individual health profiles.
Conclusion
Peptide therapy for belly fat has moved well beyond speculation. FDA-approved options like tesamorelin, semaglutide, and tirzepatide have clinical trial data involving tens of thousands of patients backing their efficacy. The science is specific: these compounds target visceral fat through defined hormonal pathways that diet and exercise alone can't fully activate.
But peptides aren't magic injections. They work best as part of a broader strategy that includes nutrition, movement, and ongoing medical supervision. Results take months, not days. Side effects are real and manageable with proper guidance. And the right peptide for one person may not be the right one for another.
The best starting point is a conversation with a physician who specializes in these protocols. For those unsure where to find one, Peptide Injections connects patients with qualified providers in minutes, cutting through the research burden and getting straight to personalized care.
Frequently Asked Questions About Peptides for Belly Fat
What is a peptide for belly fat and how does it work?
Peptides for belly fat are short chains of amino acids that mimic hormones to trigger biological responses. They target visceral fat specifically by stimulating growth hormone release (like tesamorelin) or suppressing appetite (like semaglutide). Unlike diet alone, peptides activate hormonal pathways that visceral fat cells respond to directly.
Which peptide is best for reducing visceral belly fat?
Tesamorelin is the only FDA-approved peptide specifically for visceral fat reduction, achieving approximately 11% VAT reduction versus placebo. It works by stimulating growth hormone release, which activates lipase enzymes that break down stored triglycerides in deep abdominal fat while preserving lean muscle mass.
How long does it take to see results from peptide therapy for belly fat?
With tesamorelin, measurable waist circumference reduction typically appears within 12-16 weeks, with full effect at 26-52 weeks. GLP-1 agonists like semaglutide show 5% weight loss by weeks 12-16, continuing through month 12-15. Results depend on the specific peptide, starting point, and lifestyle factors.
Are peptides for belly fat safe, and what are the common side effects?
FDA-approved peptides are generally safe when prescribed by qualified physicians. GLP-1 agonists commonly cause nausea (up to 44%), diarrhea (30%), and vomiting (24%), mostly resolving after 4-8 weeks. Growth hormone-releasing peptides may cause injection site reactions or mild joint pain. Serious risks are rare but include pancreatitis and gallstone formation.
Can I use a peptide for belly fat without diet and exercise?
Peptides work best as an accelerator, not a replacement for healthy habits. Clinical trial participants combining peptides with structured diet and exercise achieved optimal results. Without lifestyle changes, peptide therapy alone produces significantly reduced results and may lead to weight regain after discontinuation.
What is the difference between tesamorelin, semaglutide, and tirzepatide for belly fat?
Tesamorelin specifically targets visceral fat via growth hormone stimulation (11% reduction). Semaglutide reduces overall weight loss by 15% through appetite suppression. Tirzepatide, a dual GIP/GLP-1 agonist, achieves up to 22.5% weight loss but affects total body weight rather than visceral fat selectively.