A semaglutide dose chart is the single most useful reference for anyone starting GLP-1 therapy, yet most versions floating around online are either outdated or stripped of the context that actually matters. Knowing the numbers is one thing. Understanding why each dose increase happens on a specific timeline, what to expect at each stage, and how the protocol differs depending on whether the goal is blood sugar control or weight loss, that's what separates a safe, effective experience from a frustrating one.
Semaglutide prescriptions surged past 25 million in the US during 2025, according to IQVIA prescription tracking data. With that kind of demand, misinformation spreads fast. This is especially true for patients considering compounded semaglutide, where dosing protocols may differ from FDA-approved versions. Some patients escalate too quickly. Others stall at a low dose longer than necessary because they're unsure what comes next.
This guide lays out the complete week-by-week titration schedule for both Wegovy (weight management) and Ozempic (type 2 diabetes), explains how side effects shift at each dose level, and covers what to do when things don't go according to plan. Every recommendation here reflects current FDA-approved labeling and published clinical trial data, not speculation.
How Semaglutide Works and Why Gradual Dosing Matters
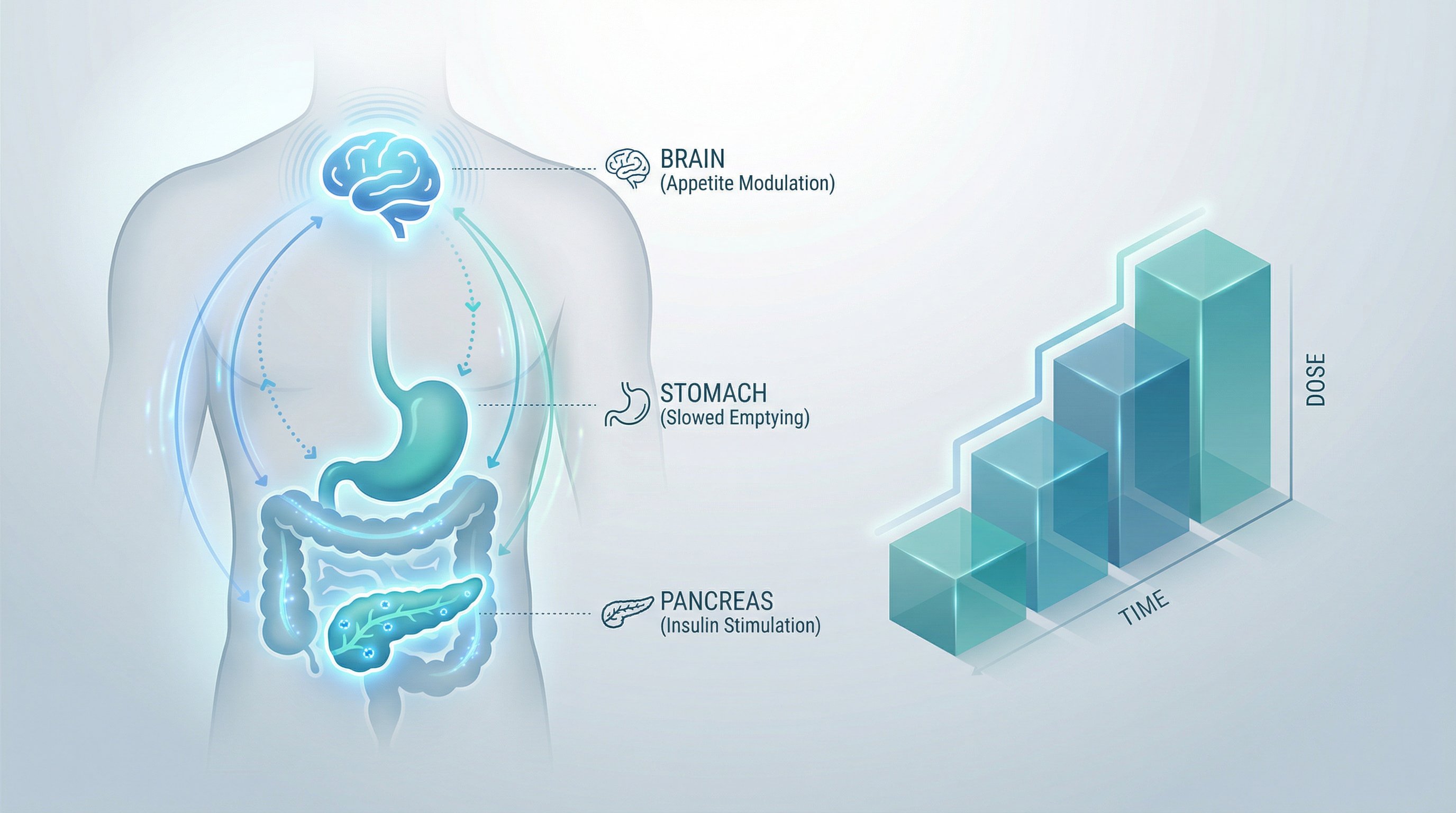
Semaglutide is a GLP-1 receptor agonist. It mimics a natural hormone called glucagon-like peptide-1, which the gut releases after eating. This hormone does three things simultaneously:
- Slows gastric emptying, so food stays in the stomach longer
- Signals the brain's appetite centers to reduce hunger
- Stimulates insulin release while suppressing glucagon, which lowers blood sugar
The drug's half-life is approximately 7 days, which is why a single weekly subcutaneous injection maintains steady blood levels. That long half-life is also precisely why gradual dosing matters so much.
When patients jump straight to a high dose, the GI tract hasn't had time to adapt. The result is often severe nausea, vomiting, or diarrhea, side effects intense enough that some people abandon treatment entirely. The STEP 1 trial, which enrolled 1,961 participants, used a structured 16-week escalation for exactly this reason. Patients who followed the gradual semaglutide dose chart achieved 14.9% mean weight loss at 68 weeks with manageable side effects, cementing semaglutide's place among the most effective peptides for weight loss.
Gradual titration gives the body's GLP-1 receptors time to adjust to sustained activation. Think of it like altitude acclimatization, climbers don't sprint to the summit because the body needs time to adapt to each new level. The same principle applies here.
The standard approach increases the dose every four weeks. Each step up is small enough that most patients tolerate it well, but meaningful enough to produce progressively stronger appetite suppression and metabolic effects.
Week-by-Week Semaglutide Dose Chart for Weight Loss
The following semaglutide dose chart reflects the FDA-approved Wegovy titration schedule for weight management. This is the protocol used in the landmark STEP clinical trial program.
| Phase | Weeks | Weekly Dose | Purpose |
|---|---|---|---|
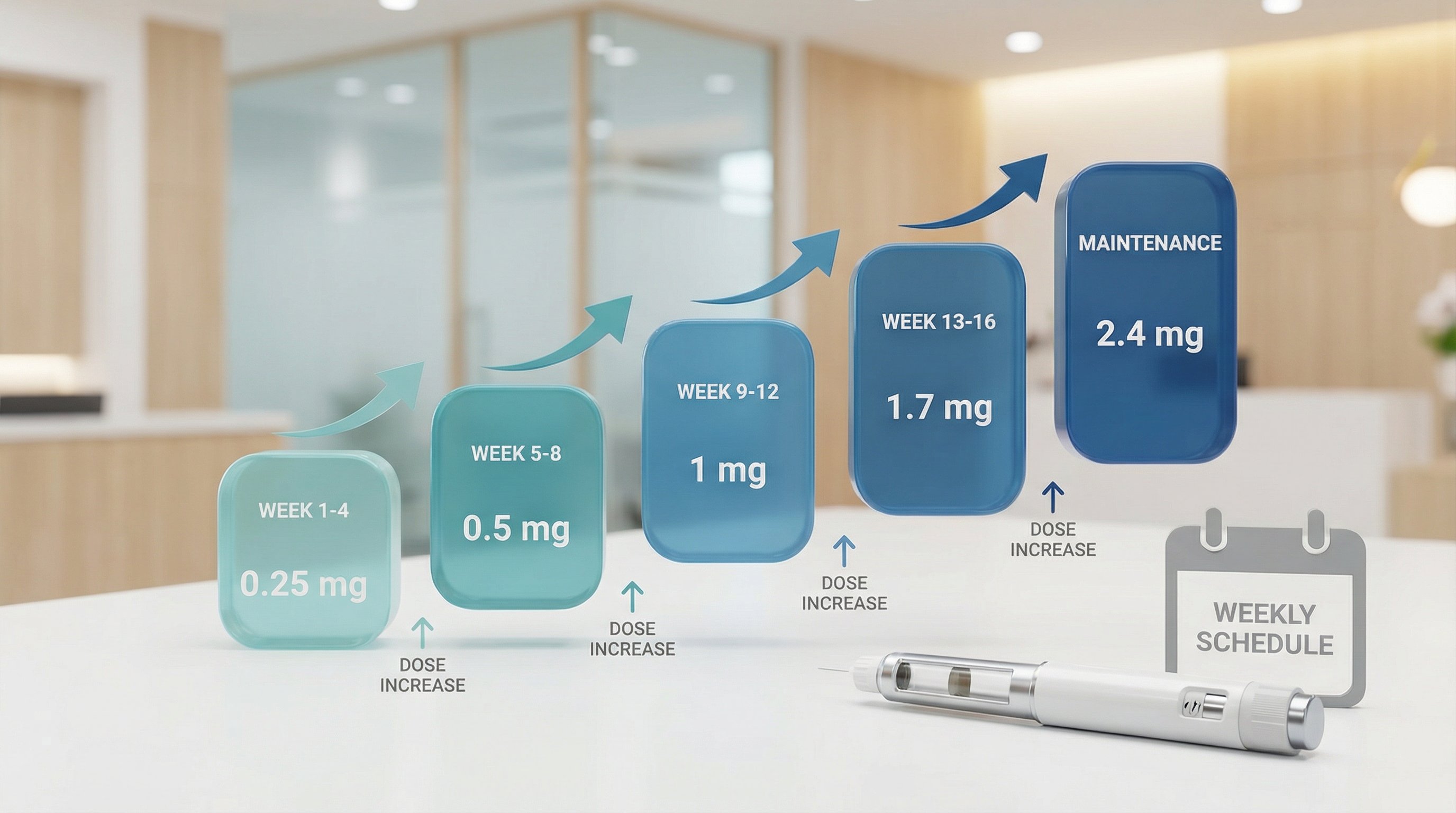
| Titration 1 | Weeks 1–4 | 0.25 mg | Initial tolerance assessment |
| Titration 2 | Weeks 5–8 | 0.5 mg | Early appetite suppression begins |
| Titration 3 | Weeks 9–12 | 1.0 mg | Noticeable hunger reduction for most patients |
| Titration 4 | Weeks 13–16 | 1.7 mg | Approaching therapeutic range |
| Maintenance | Week 17+ | 2.4 mg | Full therapeutic dose for weight loss |
Key details for each phase:
Weeks 1–4 (0.25 mg): This is not a therapeutic dose. Weight loss at this stage is minimal. The purpose is purely to let the GI system adjust. Most patients notice mild appetite changes but nothing dramatic.
Weeks 5–8 (0.5 mg): Some patients begin experiencing reduced food cravings here. Nausea is most common during this transition. Eating smaller, more frequent meals helps.
Weeks 9–12 (1.0 mg): This is where the semaglutide dose chart starts producing meaningful clinical effects. Many patients report significantly less interest in food, particularly high-fat and high-sugar options.
Weeks 13–16 (1.7 mg): Weight loss accelerates. GI side effects that appeared at earlier doses often stabilize by this point as the body has adapted over three months.
Week 17 onward (2.4 mg): The full maintenance dose. In the STEP 1 trial, participants on 2.4 mg lost an average of 33.7 pounds over 68 weeks. This dose is continued indefinitely, the STEP 5 trial confirmed weight loss is maintained at 104 weeks with ongoing treatment, but weight regain is typical after discontinuation. Patients who plateau at maintenance dose may want to explore tirzepatide vs semaglutide options.
Injection timing: Same day each week, any time of day. Patients can change their injection day as long as the last dose was given at least 2 days (48 hours) prior.
Semaglutide Dosing for Type 2 Diabetes vs. Weight Management
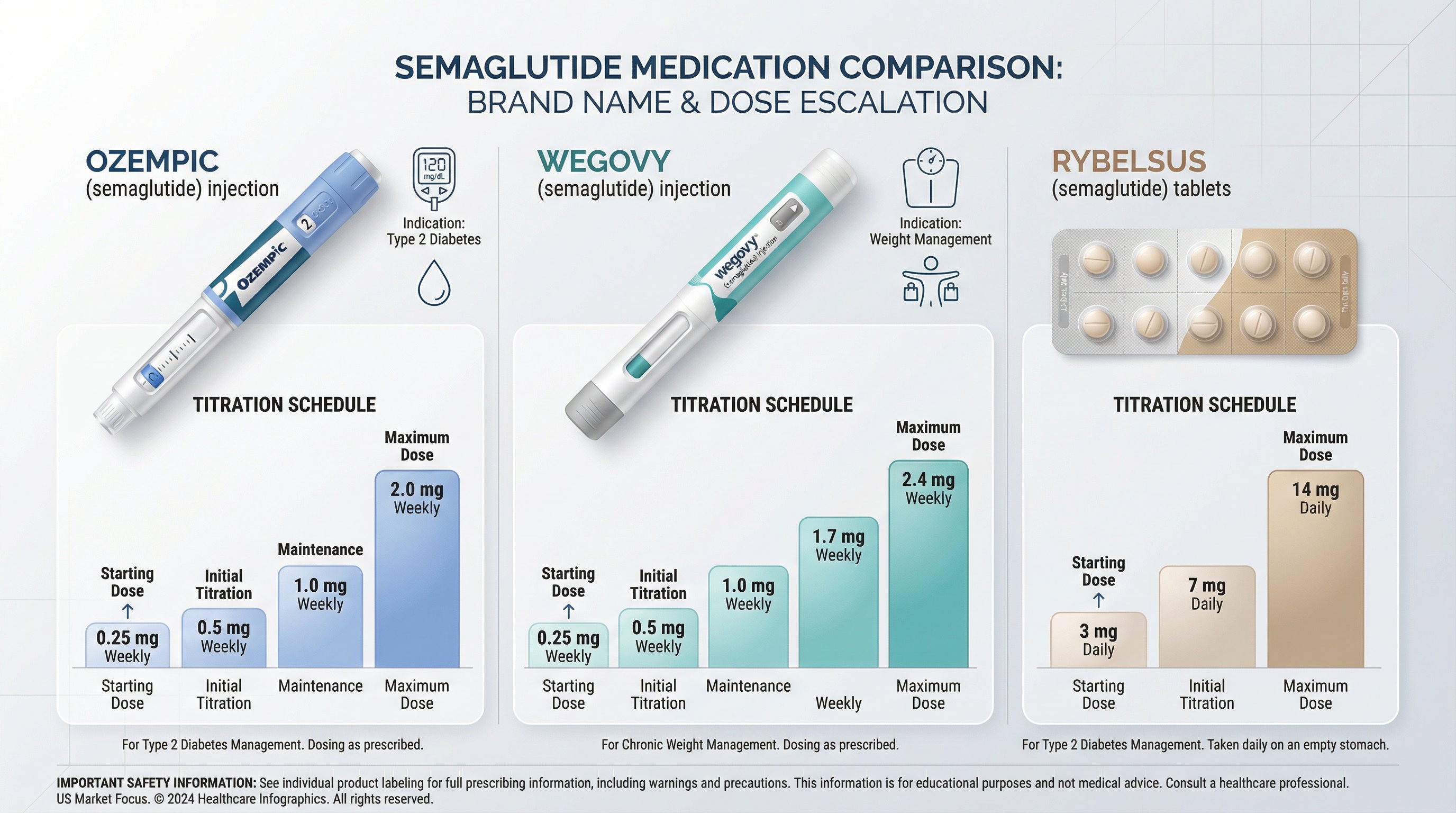
Semaglutide is FDA-approved under two brand names for two distinct indications, and the dosing protocols are not interchangeable.
Ozempic (Type 2 Diabetes)
- Starting dose: 0.25 mg weekly for 4 weeks
- Step up: 0.5 mg weekly for at least 4 weeks
- Further escalation: 1.0 mg weekly
- Maximum dose: 2.0 mg weekly
Ozempic's primary endpoint is HbA1c reduction, not weight loss. In the SUSTAIN clinical trials, the 1.0 mg dose reduced HbA1c by approximately 1.5–1.8%. The SUSTAIN-6 cardiovascular outcomes trial showed a 26% reduction in major adverse cardiovascular events and a 39% reduction in non-fatal stroke.
Wegovy (Weight Management)
- Starting dose: 0.25 mg weekly for 4 weeks
- Escalation: 0.5 → 1.0 → 1.7 → 2.4 mg (each step lasting 4 weeks)
- Maintenance dose: 2.4 mg weekly
Wegovy's titration goes higher than Ozempic because the weight loss indication requires a stronger dose. The SELECT trial (17,604 patients) demonstrated a 20% reduction in major cardiac events at the 2.4 mg dose, establishing cardiovascular benefit beyond just weight reduction.
Rybelsus (Oral Semaglutide)
There's also an oral option. Rybelsus uses a different semaglutide dose chart entirely:
- Starting dose: 3 mg daily for 30 days
- Step up: 7 mg daily for 30 days
- Maintenance: 14 mg daily
Oral semaglutide must be taken on an empty stomach with no more than 4 ounces of plain water, then patients wait at least 30 minutes before eating or taking other medications. Absorption is significantly affected by food, so this protocol is strict.
The critical distinction: a patient using Ozempic at 2.0 mg for diabetes should not assume they can switch to Wegovy at 2.4 mg without medical guidance. The formulations, titration schedules, and approved indications differ. A physician or board-certified provider should manage any transitions between products.
Common Side Effects at Each Dose Level and How to Manage Them
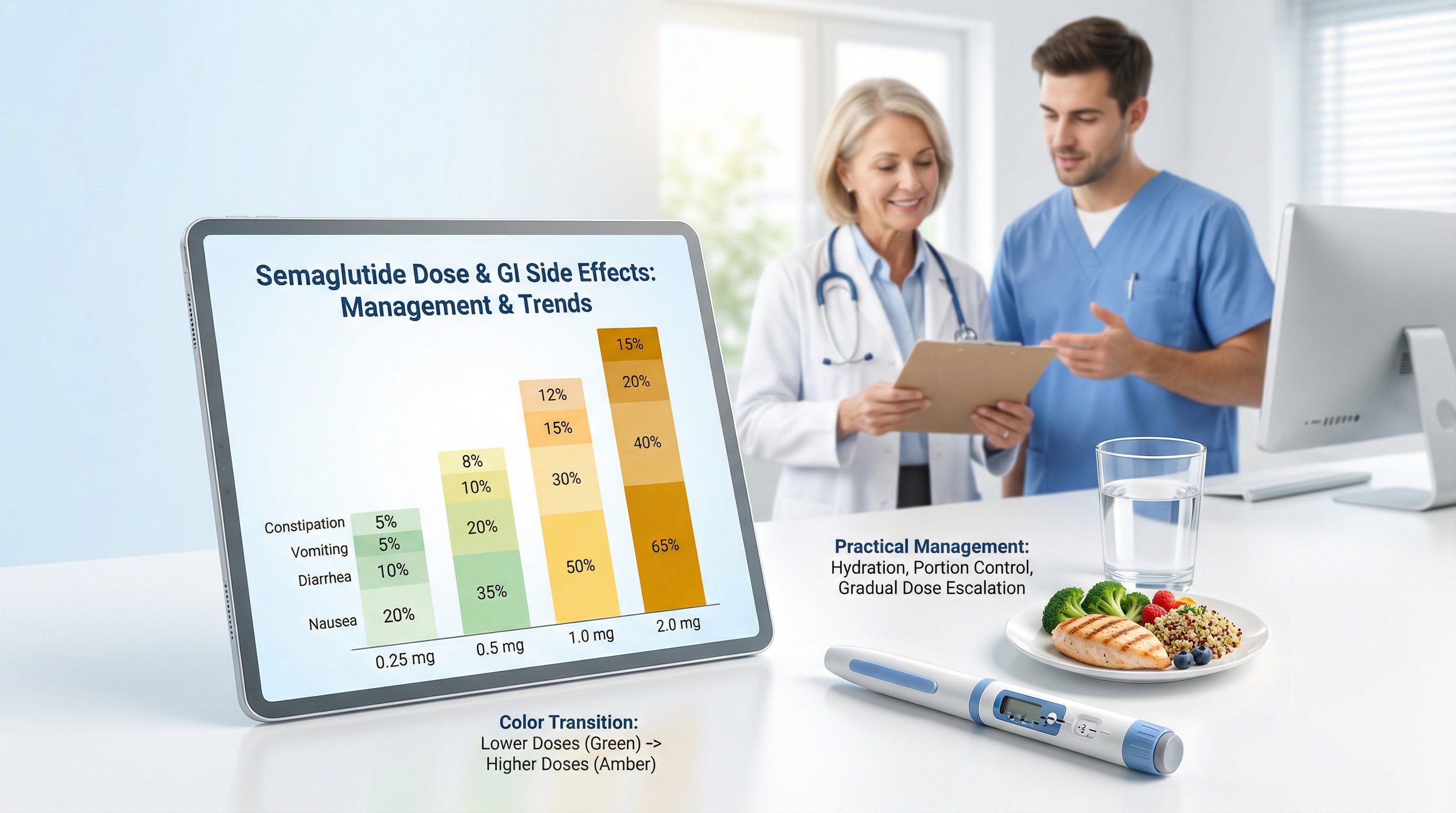
Side effects follow the semaglutide dose chart in a predictable pattern. They tend to peak during each dose increase and then improve over 1–2 weeks as the body adjusts.
GI Side Effects by Dose
Clinical trial data from the STEP program shows these approximate rates at the 2.4 mg maintenance dose:
- Nausea: Up to 44% of patients (most common complaint)
- Diarrhea: ~30%
- Vomiting: ~24%
- Constipation: ~24%
- Decreased appetite: Common but often considered a desired effect
At the lower titration doses (0.25–0.5 mg), these rates are substantially lower. Most patients who experience nausea at 0.25 mg describe it as mild and intermittent.
Dose-Specific Patterns
0.25–0.5 mg: Mild nausea, usually in the first 2–3 days after injection. Some patients feel nothing at all.
1.0 mg: This is the dose where GI side effects become more noticeable for many people. Nausea may last longer into the week. Constipation often appears here.
1.7–2.4 mg: Peak side effect intensity. Patients who escalated too quickly report the worst symptoms at these doses. But, those who followed the standard 4-week escalation schedule typically find the transition more tolerable.
Management Strategies
- Eat smaller meals. Large portions overwhelm a stomach that's emptying more slowly.
- Avoid high-fat and fried foods. These are the most common nausea triggers on semaglutide.
- Stay hydrated. Especially important if experiencing diarrhea or vomiting.
- Consider timing. Some patients report fewer symptoms when injecting in the evening before bed, sleeping through the initial nausea window.
- Slow the escalation if needed. Providers can extend any titration step beyond 4 weeks. Spending 6–8 weeks at a dose instead of 4 is a common and medically appropriate adjustment.
When to Contact a Provider
Rare but serious side effects require immediate medical attention: signs of pancreatitis (severe abdominal pain radiating to the back), symptoms of gallbladder problems (sharp upper-right abdominal pain), or allergic reactions. Semaglutide carries a boxed warning about medullary thyroid carcinoma (MTC) risk and is contraindicated in patients with a personal or family history of MTC or Multiple Endocrine Neoplasia syndrome type 2 (MEN2).
What to Do When You Miss a Dose or Hit a Weight Loss Plateau

Missed Doses
Life happens. Here's the protocol straight from the prescribing information:
- If the missed dose is within 5 days of the scheduled injection day: Take it as soon as possible, then resume the regular weekly schedule.
- If more than 5 days have passed: Skip the missed dose entirely. Take the next dose on the regularly scheduled day.
- After the missed dose: Continue with the normal schedule. Do not double up.
If multiple consecutive doses are missed, say, due to a supply shortage or travel, providers may recommend stepping back one level on the semaglutide dose chart and re-titrating. This helps avoid a spike in GI side effects from restarting at a higher dose after a gap.
Weight Loss Plateaus
Plateaus are common and don't necessarily mean semaglutide has stopped working. The body's metabolic rate adjusts to lower body weight, which naturally slows the rate of loss.
When plateaus typically occur:
- Around months 6–9 of treatment
- After 10–15% body weight loss
- During periods of reduced physical activity or dietary drift
Strategies that help:
- Confirm the dose. Some patients plateau at 1.0 or 1.7 mg and haven't yet reached the full 2.4 mg maintenance dose. Escalation may restart progress.
- Review dietary patterns. Appetite suppression can lead to unconsciously poor food choices, eating less but eating calorie-dense, low-nutrient foods.
- Add or increase resistance training. Preserving lean muscle mass keeps metabolic rate higher. Clinical trials are currently examining combinations of semaglutide with muscle-preserving compounds like enobosarm for this exact reason.
- Check adherence. Even small inconsistencies in weekly injection timing can affect blood levels.
- Discuss alternatives with a provider. For patients who plateau on semaglutide, options include tirzepatide (Zepbound), which uses a dual GIP/GLP-1 mechanism and produced 20.9% mean weight loss in the SURMOUNT-1 trial. Genetic factors like GLP1R receptor sensitivity can influence individual response, a topic a specialized provider can evaluate.
Platforms like Peptide Injections connect patients with board-certified physicians who specialize in GLP-1 therapy and can assess whether a dose adjustment, medication switch, or combination approach makes sense.
Finding Your Optimal Maintenance Dose With Medical Guidance
Not everyone needs the maximum dose. That's a critical point the standard semaglutide dose chart doesn't always make clear.
The FDA-approved maintenance dose for Wegovy is 2.4 mg, but some patients achieve their goals at 1.0 or 1.7 mg with fewer side effects. A provider evaluates several factors before deciding where on the dose chart a patient should land:
- Weight loss trajectory: If a patient is losing steadily at 1.7 mg, pushing to 2.4 mg may not be necessary.
- Side effect burden: Persistent nausea or GI discomfort at higher doses sometimes means a lower maintenance dose produces better overall outcomes because the patient can actually stay on the medication long-term.
- Metabolic markers: HbA1c, fasting glucose, and lipid panels at baseline and 12 weeks help guide decisions.
- Individual goals: A patient targeting 10% body weight loss has different dosing needs than someone aiming for 20%.
The Role of Specialized Providers
GLP-1 therapy isn't one-size-fits-all. General practitioners prescribe semaglutide frequently, but providers who specialize in peptide therapy and metabolic health bring a different level of protocol knowledge.
They understand dose-response curves, recognize when genetic factors (like GLP1R receptor variants) might explain a weak response, and know when to consider newer options like CagriSema, a combination of cagrilintide and semaglutide that produced 20.4% weight loss in the REDEFINE 1 trial, outperforming semaglutide alone.
Finding these specialists used to take hours of research. Peptide Injections simplifies this by matching patients with vetted, board-certified physicians who focus on peptide therapy protocols, typically in about 2 minutes. The platform provides personalized protocol recommendations and transparent access to providers experienced in GLP-1 dose optimization.
Ongoing Monitoring
Regardless of the maintenance dose, regular bloodwork is non-negotiable:
- HbA1c and fasting glucose at baseline and every 12 weeks
- Lipid panel at baseline and 12 weeks
- Amylase and lipase at baseline (pancreatitis screening)
- Comprehensive metabolic panel at baseline
These labs help providers catch issues early and confirm the medication is producing the expected metabolic improvements beyond just the number on the scale.
Conclusion
The semaglutide dose chart isn't just a set of numbers, it's a roadmap that, when followed correctly, produces some of the strongest weight loss and metabolic health outcomes available in medicine today. The 16-week titration from 0.25 mg to 2.4 mg exists for good reason: it balances effectiveness with tolerability.
But the chart is a starting point, not a rigid prescription. Individual responses vary based on genetics, metabolism, side effect tolerance, and goals. The patients who get the best results are the ones working with providers who understand how to personalize the protocol.
Whether someone is starting their first 0.25 mg injection or troubleshooting a plateau at 1.7 mg, the right medical guidance makes the difference. Platforms like Peptide Injections exist specifically to close that gap, connecting patients with specialized physicians who treat GLP-1 optimization as their core focus, not an afterthought.
Frequently Asked Questions About Semaglutide Dosing
What is the standard semaglutide dose chart for weight loss?
The FDA-approved Wegovy titration schedule starts at 0.25 mg weekly (weeks 1–4), escalating every 4 weeks to 0.5 mg, 1.0 mg, 1.7 mg, then 2.4 mg maintenance (week 17+). This 16-week gradual progression balances effectiveness with tolerability and allows the GI tract to adapt.
Why does semaglutide dosing increase gradually instead of jumping to the full dose?
Semaglutide's 7-day half-life means gradual dosing prevents severe GI side effects like nausea and vomiting. The STEP 1 trial showed that patients following the standard 4-week escalation achieved 14.9% mean weight loss with manageable side effects, while rapid escalation often causes intolerable symptoms that lead to treatment discontinuation.
What is the difference between Ozempic and Wegovy dosing?
Ozempic (type 2 diabetes) reaches a maximum of 2.0 mg weekly, while Wegovy (weight management) escalates to 2.4 mg. Ozempic's primary endpoint is HbA1c reduction; Wegovy's is weight loss. The formulations and titration schedules differ—never switch between products without medical guidance.
How long do semaglutide side effects last at each dose level?
Side effects typically peak during each dose increase and improve over 1–2 weeks as the body adapts. At 0.25–0.5 mg, nausea is usually mild and intermittent. At 1.0–1.7 mg, GI effects become more noticeable but are manageable with dietary adjustments like eating smaller meals and avoiding high-fat foods.
What should I do if I miss a semaglutide injection?
If the missed dose is within 5 days of your scheduled injection, take it as soon as possible and resume your regular weekly schedule. If more than 5 days have passed, skip that dose and take your next injection on the regularly scheduled day. Never double up on doses.
Why do weight loss plateaus occur on semaglutide, and how do you overcome them?
Plateaus are common after 6–9 months or 10–15% weight loss as metabolic rate adjusts to lower body weight. Strategies include confirming you've reached the full 2.4 mg maintenance dose, reviewing dietary patterns for calorie-dense foods, adding resistance training to preserve lean muscle, and consulting a specialized provider about alternatives like tirzepatide if needed.